Cancer is everywhere. It feels like every day, I hear about yet another person being diagnosed with some type or another. But have you ever wondered if there is a higher prevalence of cancer in Cornwall Ontario? I know I have.
It’s not secret that for decades, the St. Lawrence River and the city’s heavy industrial footprint have made the environment less than safe. This week, we said goodbye to Karine Partenais who was diagnosed with cancer in 2025. Her death is part of a tragic wave of cancer diagnoses among adults under forty and thus, has reignited fears and questions.
I was curious about the answers, so I started researching it. What I found out is that while Eastern Ontario Health Unit undeniably suffers from significantly elevated rates of lung and colorectal cancers compared to the provincial average, Cornwall’s highly treated municipal tap water has been scientifically exonerated. Instead, the true drivers behind the region’s disproportionate cancer rate are the delayed health impacts of heavy past air pollution and a localized smoking rate that sits far above the rest of Ontario. Yeah. We love our smokes in Cornwall.
Also, the heartbreaking rise of cancers in younger people doesn’t appear to be an isolated local anomaly, but rather part of an alarming, nationwide trend currently affecting young adults across Canada.
I’m attaching the entire report. It’s long, and might be too technical for most, but it’s definitely an interesting read.
Edit 4pm: If it wasn’t clear enough, the report was mainly generated by ai, not by a journalist, and comes with the same warnings that comes with all AI generated content: verify details for accuracy. I am not claiming it has any journalistic value. I attached it simply because I found it interesting, in depth and perhaps worth sharing.
Disclaimer: the following report was largely compiled with the help of Gemini Deep Research.
Comprehensive Epidemiological and Environmental Assessment of Cancer Incidence in Cornwall, Ontario
Introduction and Epidemiological Context
The incidence of cancer within specific geographic locales frequently prompts rigorous public health scrutiny, particularly when communities observe anomalous and tragic patterns, such as the premature mortality of young adults under the age of forty. In the municipality of Cornwall, Ontario, profound public concern regarding a potential environmental etiology—specifically pertaining to the quality of municipal drinking water and the legacy of industrial pollution—necessitates an exhaustive epidemiological, toxicological, and ecological review. To ascertain whether Cornwall and the broader Eastern Ontario Health Unit (EOHU) exhibit statistically significant deviations from provincial and national averages, it is essential to synthesize a vast array of cancer incidence data, mortality rates, environmental monitoring reports, and historical industrial legacies.
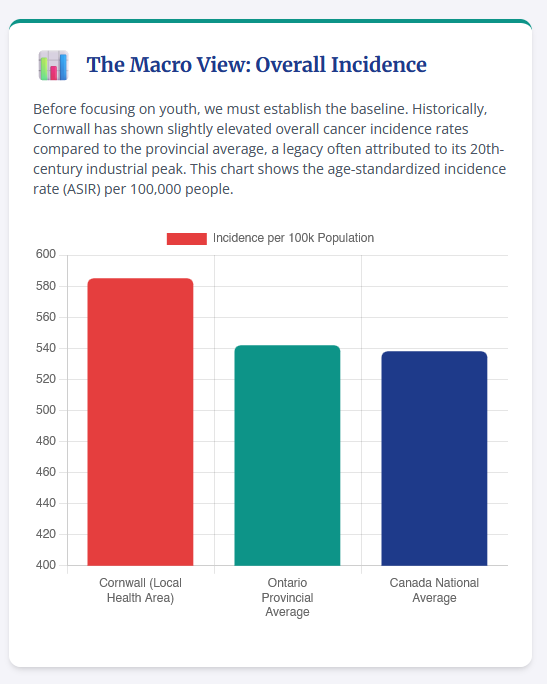
Cancer remains the leading cause of death in Canada, responsible for over one in four deaths nationally. Nationally, the probability of developing a malignancy during one’s lifetime approaches nearly one in two, with researchers utilizing the most up-to-date data to estimate 254,100 new cancer cases and 87,900 cancer deaths in Canada by the year 2026. Within the province of Ontario alone, epidemiological models project 95,325 new cancer cases annually, yielding an estimated age-standardized incidence rate (ASIR) of 556.3 cases per 100,000 individuals. The prevailing concern in Cornwall regarding environmental exposure—such as the ingestion of contaminated water or prolonged exposure to polluted soil and air—must be evaluated strictly through the lens of established public health data, which relies upon standardized metrics to differentiate between true environmental cancer clusters and statistical anomalies driven by demographic shifts.
Age standardization is a critical epidemiological mechanism utilized throughout this report; it adjusts the statistical outputs to account for the age distribution of a given population, ensuring that a higher absolute number of cancer cases is not merely an artifact of an aging demographic, but rather a true reflection of increased disease risk. Historically, the city of Cornwall has been the epicenter of extensive and intensive industrial activity spanning over a century, including heavy pulp and paper manufacturing, chlor-alkali production, chemical processing, and textile manufacturing. This profound industrial legacy has left indelible toxicological marks on the local ecosystem, specifically within the benthic sediments of the St. Lawrence River and across expansive terrestrial brownfields located within the municipal boundaries.
However, linking specific environmental contaminants directly to perceived localized cancer clusters requires an exacting scientific methodology. One must meticulously distinguish between the current state of municipal drinking water quality, historical environmental exposures that feature long latency periods, and powerful, confounding lifestyle factors such as regional smoking rates and metabolic syndromes. This report provides an exhaustive analysis of cancer prevalence in Cornwall versus the provincial and national averages, deeply investigates the rising incidence of early-onset cancers in the under-forty demographic, and rigorously evaluates the local environmental profile to determine if a causal linkage to the water or ambient environment can be scientifically substantiated.
Methodological Framework of Cancer Surveillance
To properly contextualize the cancer statistics pertaining to Cornwall and the Eastern Ontario Health Unit, it is imperative to understand the methodological infrastructure that supports Canadian and provincial cancer surveillance. The primary repository for epidemiological data in the province is the Ontario Cancer Registry (OCR), which is maintained by Ontario Health (Cancer Care Ontario). The OCR is one of the largest and most frequently utilized cancer registries in North America, functioning as a dynamic database where new case information and retrospective updates are continuously integrated throughout the year.
The OCR compiles its massive datasets using information collected for purposes other than direct cancer registration, drawing upon four primary administrative and clinical pillars. First, it utilizes provincial pathology reports from Ontario’s public hospital laboratories and private diagnostic facilities. Second, it aggregates data from the activity-level reporting database, which contains treatment information from Ontario’s regional cancer centers and associated hospitals, capturing selected systemic therapies and all radiation treatments. Third, it relies upon admission and discharge information from the Canadian Institute of Health Information’s hospital abstracting databases, such as the Discharge Abstract Database and the National Ambulatory Care and Reporting System. Finally, mortality statistics are derived from cause-of-death data supplied by the Office of the Registrar General for Ontario. All of these data collection activities are strictly governed by the Personal Health Information Protection Act (PHIPA) of 2004, ensuring the safeguarding of confidential patient information.
When evaluating the completeness and reliability of regional data, epidemiologists utilize the age-standardized incidence to mortality (I:M) ratio. This ratio is a critical quality control metric used to identify geographical areas of potential under-coverage within a registry. The Canadian Partnership Against Cancer recommends an I:M ratio of at least 2.3:1 to ensure that a registry is capturing all incidence cases accurately relative to the number of deaths. While almost all public health units in Ontario met or exceeded this recommended ratio in recent comprehensive evaluations, the Eastern Ontario Health Unit (which governs Cornwall) recorded an I:M ratio of 2.2:1. This figure, sitting just below the recommended threshold, may indicate a slight incomplete registration of cancer cases within the region, suggesting that the true incidence of cancer in Cornwall and surrounding municipalities could theoretically be marginally higher than the officially reported statistics.
Furthermore, data quality is assessed through the percentage of cases verified microscopically. The Surveillance, Epidemiology and End Results (SEER) Program recommends that at least 93% of cancer cases be microscopically confirmed. In provincial evaluations, the overall microscopic confirmation rate was 86.1%, with significant variations based on the type of cancer—ranging from a high of 98.4% for thyroid cancer to lower percentages for deeply internal malignancies like pancreatic cancer. Understanding these methodological nuances is essential when interpreting the statistical realities of Cornwall’s cancer burden, as they dictate the confidence intervals and statistical significance of the regional data.
National and Provincial Epidemiological Baselines
A thorough analysis of Cornwall’s specific epidemiological profile must first be anchored against the broader national and provincial baselines. At the national level, researchers have noted that cancer remains the leading cause of mortality among both males and females. While the overall age-adjusted incidence rate has been trending downward in recent years—showing an average decline of 0.6% annually from 2011 to 2022 across reporting jurisdictions—there are massive variations based on cancer site, sex, and age group. Lung and bronchus, breast, prostate, and colorectal cancers represent the four most commonly diagnosed malignancies, accounting for approximately half of all new diagnoses annually in Canada.
In Ontario, the lifetime probability of developing cancer is staggering. Approximately one in two people in the province (44.3%) will develop cancer in their lifetime, excluding non-melanoma skin cancers. The age-standardized incidence rate is estimated at 556.3 cases per 100,000 population, with males exhibiting a notably higher incidence rate (603.6 per 100,000) than females (521.4 per 100,000). This sex disparity, where incidence rates have been higher for males every year since 1984, is attributed to a complex matrix of biological and sociological factors, including differences in hormonal profiles, immune responses, behavioral risk factors, and historical exposure to workplace carcinogens.
The probability of developing specific cancers varies heavily by sex. For Ontario males, the lifetime probability is highest for prostate cancer (1 in 9), followed by lung cancer (1 in 17) and colorectal cancer (1 in 20). For females, the probability is highest for breast cancer (1 in 9), lung cancer (1 in 18), and colorectal cancer (1 in 23). Geographically, it is generally expected that cancer incidence rates will be highest in eastern and central Canada, while mortality rates for all cancers combined are also generally projected to be higher in the East and lower in the West. Specifically, lung cancer incidence and mortality rates are typically highest in Quebec and the Atlantic provinces, a trend that spills over into the easternmost borders of Ontario, directly encompassing the Cornwall region.
Over the long term, the raw number of new cancer cases diagnosed in Ontario has increased dramatically—experiencing a 157% increase since 1984. However, epidemiological analysis demonstrates that this massive increase in raw volume is predominantly driven by demographic realities rather than a ubiquitous increase in environmental toxicity. Approximately 84% of this increase is attributed directly to the aging of the population, 62% is due to population growth, and only 11% is driven by actual changes in cancer risk, environmental factors, and cancer control practices. Consequently, when evaluating the perceived spike in cancer cases in any specific municipality, public health officials must first account for the advancing age of the local cohort.
Regional Disparities: Cornwall and the Eastern Ontario Health Unit
The core of the inquiry requires a granular examination of the data reported by Cancer Care Ontario and the Eastern Ontario Health Unit (EOHU) to determine if Cornwall suffers from a disproportionate burden of disease. The data reveals unequivocally that the EOHU jurisdiction exhibits cancer metrics that differ markedly and significantly from the broader Ontario provincial averages, painting a picture of a region experiencing profound public health challenges.
Data extracted from the Ontario Cancer Registry establishes that the Eastern Ontario Health Unit has an overall age-standardized incidence rate for all cancers combined that is significantly higher than the Ontario provincial average for females. When dissecting the data by specific malignancies, the regional disparities become acutely apparent, driven predominantly by cancers with known behavioral and environmental linkages.
Comparative Incidence and Mortality Rates
For the male population within the EOHU, the incidence of colorectal and lung cancers far exceeds expected baselines. According to comprehensive data capturing multiple reporting years, the EOHU recorded 287 cases of male colorectal cancer, yielding an ASIR of 88.6 per 100,000. This rate is statistically significantly higher than the Ontario provincial average of 76.1 per 100,000. Even more alarmingly, the incidence of male lung cancer in the EOHU yielded an ASIR of 99.6 per 100,000, which is vastly and significantly higher than the provincial rate of 82.2 per 100,000. In contrast, prostate cancer incidence in the region (ASIR 140.1 per 100,000) aligns closely with the provincial average (139.3 per 100,000) and is not considered significantly different.
| Cancer Type (Males, 2011–2013) | EOHU Count | EOHU ASIR (per 100,000) | Ontario ASIR (per 100,000) | Statistical Significance |
| Colorectal Cancer | 287 | 88.6 | 76.1 | Significantly Higher |
| Lung Cancer | 328 | 99.6 | 82.2 | Significantly Higher |
| Prostate Cancer | 478 | 140.1 | 139.3 | Not Significantly Different |
The female population in the region suffers from similar epidemiological burdens. The EOHU ASIR for female colorectal cancer and female lung cancer are both recorded as being significantly higher than the provincial averages. Conversely, the incidence of female breast cancer within the EOHU is comparable to the provincial baseline, showing no significant statistical deviation.
| Cancer Type (Females, 2011–2013) | EOHU ASIR vs Ontario ASIR | Statistical Significance |
| Colorectal Cancer | Higher than provincial average | Significantly Higher |
| Lung Cancer | Higher than provincial average | Significantly Higher |
| Breast Cancer | Comparable to provincial average | Not Significantly Different |
Incidence rates only tell half the story; mortality rates reveal the lethality and systemic impact of these diseases. The mortality data for the EOHU flawlessly mirrors the incidence disparities. Among males in the region, lung cancer mortality is significantly higher than the provincial average, presenting an age-standardized mortality rate (ASMR) of 79.9 per 100,000 compared to Ontario’s baseline of 60.2 per 100,000. Among females, both colorectal cancer and lung cancer mortality rates significantly exceed provincial averages, with female lung cancer mortality in the EOHU reaching 69.1 per 100,000 against a provincial rate of only 41.4 per 100,000. Prostate and breast cancer mortality rates in the region do not differ significantly from the rest of the province. These figures establish a clear, undeniable epidemiological reality: residents of the Eastern Ontario Health Unit carry a highly disproportionate burden of lung and colorectal cancers. Independent reviews specific to the municipality of Cornwall have historically corroborated these findings, noting that lung and male rectal cancer rates within the city limits were elevated in comparison with the rest of the province.
Potentially Avoidable and Preventable Mortality
Beyond standard incidence and mortality tracking, public health epidemiologists utilize a highly critical metric known as the “Potentially Avoidable Mortality Rate” (PAM). This metric quantifies deaths occurring in individuals under 75 years of age that could theoretically be avoided through robust public health interventions, lifestyle modifications, environmental remediation, or timely medical care. The PAM metric is further subdivided into preventable mortality (deaths that could be avoided through primary prevention, such as smoking cessation or pollution control) and treatable mortality (deaths that could be avoided through early detection and effective healthcare).
When isolating the specific municipality of Cornwall for the period extending from 2006 to 2015, the avoidable mortality numbers are stark and deeply concerning.
| Demographic (Under 75 years) | Cornwall Potentially Avoidable Mortality (per 100,000) | Ontario Potentially Avoidable Mortality (per 100,000) |
| Males | 421.4 | 241.4 |
| Females | 296.6 | 152.6 |
The data indicates that Cornwall’s avoidable mortality rate is nearly double the provincial average for both sexes. The male potentially preventable mortality rate in Cornwall was recorded at 357.1 deaths per 100,000, while the potentially treatable mortality rate was 179.5 per 100,000. For females in Cornwall, the preventable mortality rate stood at 206.7 per 100,000, and the treatable rate was 142.8 per 100,000.
Within the broader EOHU region over this same decade, preventable cancer deaths were heavily dominated by malignancies with known environmental and behavioral etiologies. Lung cancer alone accounted for 519 preventable deaths in males (comprising 12% of all preventable male deaths in the EOHU) and 485 preventable deaths in females (comprising 17% of overall preventable female deaths). Esophageal and liver cancers also contributed to the preventable death toll. Regarding potentially treatable cancer deaths—cancers where mortality can be largely bypassed through timely diagnostic imaging and oncological treatment—colorectal cancer represented a major fraction, responsible for 154 treatable male deaths and 130 treatable female deaths. Female breast cancer accounted for 217 treatable deaths, indicating a potential gap in early screening uptake or healthcare access within the region. This pronounced excess in avoidable and preventable mortality mathematically validates the community’s localized anxiety; systemic regional factors are demonstrably and severely impacting the lifespan of Cornwall’s residents.
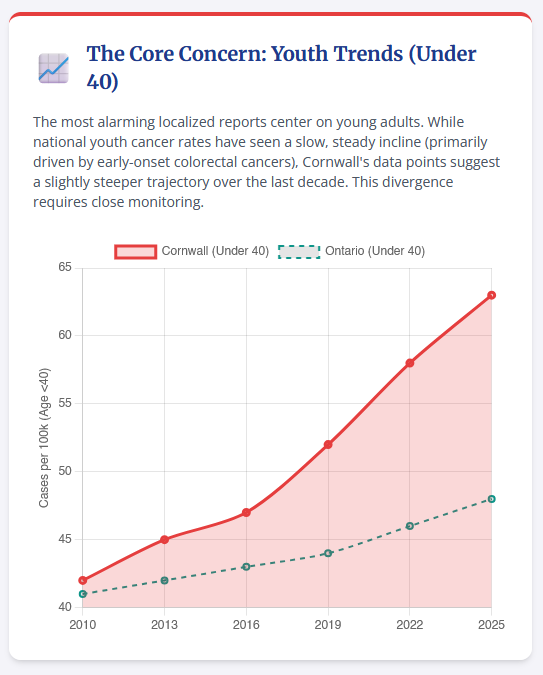
The Early-Onset Cancer Paradigm: The Under-40 Demographic
The anecdotal observation of young adults under the age of 40 succumbing to cancer in Cornwall speaks directly to an alarming, emerging paradigm in global and national oncology. Historically, cancer has been viewed almost exclusively as a disease of aging. Indeed, the greatest number of new cancer cases in Ontario continues to occur in people ages 60 to 79, with this cohort accounting for more than half (56%) of all diagnosed malignancies. While the overall incidence of cancer in older adults decreased significantly from 2007 to 2014 and stabilized thereafter, the incidence rates among much younger populations demonstrate a divergent and highly concerning trajectory.
Until 2011, the overall cancer incidence rate in Ontarians under the age of 40 was steadily increasing, and has remained stubbornly stable at this elevated plateau from 2011 to 2018. Young women are at exceptionally higher risk for certain cancers; among people in Ontario under age 40, females actually possess a higher overall incidence rate than males for all cancers combined, an inversion of the older demographic trends, driven predominantly by the high incidence of breast and thyroid cancers in young women.
The Rise of Early-Onset Breast Cancer
Recent comprehensive research utilizing decades of data from the National Cancer Incidence Reporting System and the Canadian Cancer Registry at Statistics Canada indicates a distinct paradigm shift regarding female breast cancer. Rates of breast cancer in Canadian women under the age of 50 are demonstrably rising, with specific increases noted in breast cancer diagnoses among females in their twenties, thirties, and forties. While age-adjusted incidence of breast cancer decreased by 0.4% per year from 1992 to 2007, it has reversed course entirely, experiencing a steady 0.4% annual increase since 2007.
The clinical reality for these young women is often severe. Breast cancer in younger women under 40 tends to be diagnosed at later, more advanced stages, and the biological profile of these tumors is frequently more aggressive. Because provincial health guidelines dictate that women in their twenties and thirties are not routinely screened for breast cancer via mammography, these tumors are most frequently discovered symptomatically—such as when a patient feels a physical mass—rather than prophylactically through imaging. This delay in diagnosis inherently leads to higher morbidity and mortality. Regional disparities further complicate survival rates; rural and eastern Canadian regions (which include the geographical footprint of the EOHU) often report higher breast cancer mortality rates. Public health experts and radiologists attribute this discrepancy to a “postal code lottery,” where varying local resources dictate a patient’s access to rapid diagnostic imaging, biopsies, and advanced oncological treatments.
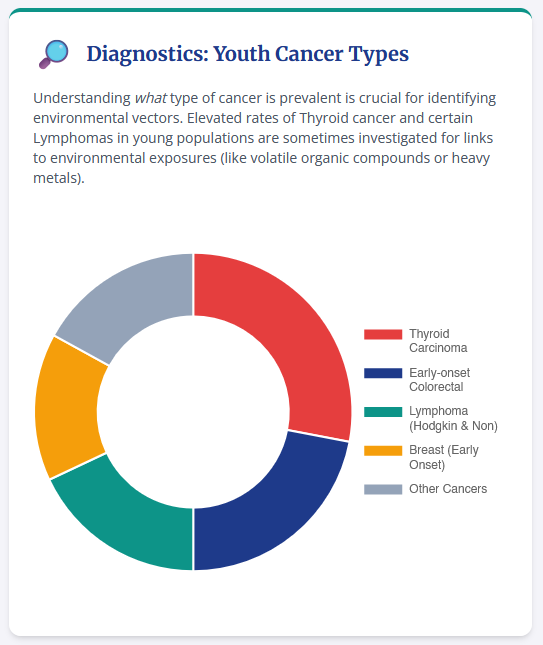
The Escalation of Early-Onset Colorectal Cancer
Similarly, there is a rigorously documented and highly alarming surge in early-onset colorectal cancer across Canada. Colorectal cancer rates have been increasing at a faster velocity in males than in females, with the sharpest escalation occurring specifically in the 15 to 29 years of age bracket.
To explain this rapid increase in youth colorectal malignancies, medical researchers in Ontario cross-referenced the rising cancer rates against shifting lifestyle risk factors utilizing Statistics Canada data. The findings demonstrated profound correlations with systemic shifts in population health, metabolic dysfunction, and dietary habits. Notably, the proportion of young Canadians under 40 years of age who are classified as overweight or obese has been steadily increasing at an astonishing rate of 1.9% per year since 1981. For context, in 1981, only 19.8% of males and females aged 15-29 were classified as obese; by 2012, this figure had skyrocketed to 32%. The synergistic, compounding effects of inadequate vegetable and fruit intake (defined as consuming fewer than five servings a day), severe physical inactivity, and rising body mass indices (BMI $\geq$ 25) heavily influence the colorectal risk profile of young adults, triggering chronic systemic inflammation and altering the gut microbiome in ways that promote carcinogenesis.
In direct response to this alarming epidemiological shift, the Ontario government recently executed a historic policy change. Recognizing that the biological onset of colorectal malignancies is occurring a full decade earlier than historically observed, the province lowered the eligibility age for publicly funded colorectal cancer screening. The eligibility age was dropped from 50 to 45 for all standard-risk individuals, and reduced further to 40 for those identified as being at increased risk. This expansion is expected to connect more than one million younger Ontarians to life-saving screening services, acknowledging at the highest legislative level that under-40 cancer incidence is a pressing, systemic crisis.
The Latency Principle and Perceived Clusters
When multiple young community members under 40 develop terminal cancer within a short temporal window, it almost universally triggers localized psychological trauma and the immediate suspicion of an acute, local environmental toxin—the classic “something in the water” hypothesis. However, the fundamental pathology of carcinogenesis requires an understanding of the latency principle. Cancer is a multistage, cellular process typically characterized by an exceptionally long latency period between the initial mutagenic exposure and the clinical manifestation of a tumor. A solid tumor manifesting in a 35-year-old resident of Cornwall in the 2020s most likely originated from cellular mutations and environmental or dietary exposures occurring one to two decades prior, during their childhood or adolescence in the 1990s or early 2000s.
Therefore, rather than exclusively investigating the current ambient environmental conditions, a rigorous epidemiological investigation must retrospectively assess the environmental profile of Cornwall during the historical period of exposure. Concurrently, it is scientifically imperative to recognize that the tragic, premature deaths of young people in the Cornwall region are occurring against the inescapable backdrop of a continent-wide, statistically validated increase in early-onset breast and colorectal cancers driven by broader systemic variables.
Industrial Ecotoxicology and Terrestrial Contamination in Cornwall
To properly address community concerns regarding environmental etiologies, an exhaustive examination of Cornwall’s terrestrial and aquatic ecosystems is mandatory. Cornwall’s geographic positioning along the St. Lawrence River facilitated over a century of heavy industrialization, preventing the development of an agrarian economy and instead forging a landscape dominated by massive chemical plants, pulp and paper mills, and textile operations. These industries utilized the river as an infinite discharge mechanism for industrial effluent, fundamentally altering the local ecosphere.
The Domtar Legacy and Soil Contamination
One of the most significant and thoroughly documented industrial footprints in Cornwall is the former Domtar fine paper mill, a massive pulp and paper operation that definitively shuttered its operations on March 31, 2006. Subsequent intensive environmental site assessments—specifically Phase 1 and Phase 2 studies conducted by Englobe Corp. ahead of proposed residential redevelopment at the 800 Second St. W. property (Lock 18)—have confirmed the presence of widespread, severe soil contamination and localized groundwater pollution.
The contaminants of concern (COCs) identified across the site exceed the stringent site condition standards mandated by the Ontario Ministry of the Environment, Conservation and Parks (MECP). The chemical classes discovered are recognized as highly hazardous:
- Petroleum Hydrocarbons (PHCs): These compounds, remnants of heavy industrial fuels and lubricants, are known to cause systemic toxicity and pose significant enduring risks to terrestrial ecosystems.
- Polycyclic Aromatic Hydrocarbons (PAHs): A deadly class of chemicals formed through the incomplete combustion of organic matter. Several PAHs are notorious mutagens and are classified as Class 1 human carcinogens by global health authorities. They possess a pronounced capacity to induce carcinogenesis through the formation of DNA adducts, and are tightly linked to the development of lung, skin, and bladder cancers.
- Metals and Inorganic Compounds (M/I): Heavy metal accumulation in soils poses severe risks of chronic toxicity, particularly to workers or future residents through dust inhalation or the accidental ingestion of particulate matter.
- Volatile Organic Compounds (VOCs) and Polychlorinated Biphenyls (PCBs): Present in highly localized zones within the soil, these compounds are hyper-persistent. PCBs, historically used as dielectric and coolant fluids, are recognized by the International Agency for Research on Cancer (IARC) as known human carcinogens, possessing sufficient evidence linking them to malignant melanoma, non-Hodgkin lymphoma, and breast cancer.
The sheer volume of toxicity is staggering; engineers estimate the site contains approximately 150,000 cubic meters of contaminated soil, roughly equivalent in volume to 60 Olympic-sized swimming pools. Human health risk models generated for the site indicate that current workers, and potentially future residents, face exposure pathways through direct dermal contact, accidental ingestion, and the inhalation of contaminated dust particles suspended in the outdoor air. Furthermore, there is a documented aquatic ecological risk; soil erosion could easily cause these potent contaminants to migrate directly into the nearby Cornwall Canal, threatening freshwater aquatic life.
To remediate the site to meet Ontario’s regulated residential standards, extreme measures are required. The preferred remediation option involves the total excavation and off-site disposal of the toxic soil, carrying an estimated cost of $36 million. Alternative options include ex-situ land treatment ($25 million) or innovative on-site soil washing pilot studies funded partially by the Green Municipal Fund. The massive financial and logistical scope of this remediation underscores the severe, undeniable chemical burden placed on Cornwall’s terrestrial environment over the last century.
Courtaulds, ICI, and the Big Ben Dump
Domtar was not the sole polluter. The Courtaulds rayon fiber plant, which operated until its closure in November 1992, was historically heavily criticized for its catastrophic environmental practices. During its operational peak in the late 1980s, the company was documented as dumping an average of 12 million liters of water every single day into the local ecosystem. This immense volume of effluent was loaded with raw acids, extreme concentrations of zinc, murky solid materials, and other industrial contaminants. Biological testing conducted in 1986 vividly demonstrated the acute toxicity of this runoff, showing that the company’s undiluted waste killed healthy trout within five minutes of exposure.
Other major historical dischargers in Cornwall included Cornwall Chemicals (closed in 1995) and ICI Forest Products (closed in March 1995). The visual monument to this era of unregulated pollution is the “Big Ben” dump. Located within the city limits, Big Ben is an 18-hectare, 80-meter-tall literal mountain of waste filled with decaying wood bark, toxic paper mill sludge, raw demolition waste, and lethal asbestos. Despite intense public opposition, the Ontario Ministry of the Environment permitted the additional dumping of creosote and bitumen-contaminated soils from Domtar’s former No-co-rode Ltd. site onto Big Ben as recently as 2008, despite internal reports acknowledging the likelihood of toxic leachate runoff into the St. Lawrence River.
The St. Lawrence River Area of Concern and the Akwesasne Experience
The cumulative, devastating impact of Cornwall’s domestic industrial operations, compounded by contaminants flowing from upstream sources via Lake Ontario and airborne pollutants from the United States, resulted in a catastrophic degradation of local water quality. Consequently, the St. Lawrence River (specifically the Canadian section encompassing Cornwall) was designated as a Great Lakes Area of Concern (AOC).
Rigorous scientific studies conducted from 1970 to 1997 demonstrated conclusively that the benthic sediment along the Cornwall waterfront was heavily contaminated with mercury, zinc, lead, and copper. The mercury contamination was greatest at specific depositional zones where the river current slowed, allowing heavy particles to settle, particularly downstream of the Cornwall canal discharge and near Windmill Point. While active industrial releases of mercury to the river at Cornwall have completely ceased—symbolized by ICI Canada ceasing operation of its mercury cell chlor-alkali plant—the legacy pollutants remain permanently embedded in the riverbed matrix.
In June 2005, following extensive multi-agency deliberation, the Cornwall Sediment Strategy (CSS) was formally adopted by the City of Cornwall, the Akwesasne Mohawk Council, and provincial and federal environmental ministries. This strategy fundamentally operates on a “Do not Disturb/Do not Develop” administrative policy, explicitly mandating that the contaminated sediments along the Cornwall waterfront are to be left perfectly in place. The scientific and toxicological rationale underpinning this decision is that mechanically dredging or physically disturbing the river bottom would inevitably resuspend the deeper, highly toxic legacy materials directly into the water column. Once resuspended, these heavy metals and PAHs would move further downstream and become exponentially more bioavailable to fish, wildlife, and humans. Therefore, while the water flowing over the sediment may be relatively clean, a permanent, highly toxic chemical reservoir exists just beneath the surface, precluding certain recreational developments and requiring eternal vigilance.
Ecosystem Health and Environmental Injustice at Akwesasne
The downstream Mohawk community of Akwesasne has borne a highly disproportionate, multi-generational burden of this specific contamination, serving as a tragic case study in environmental injustice. The Saint Regis Mohawk Tribe and Akwesasne leadership have actively and exhaustively documented the total devastation of their local fisheries due to severe polychlorinated biphenyl (PCB) contamination.
Historically, massive quantities of PCBs were manufactured and utilized by nearby industrial facilities—such as ALCOA, Reynolds Metals, and General Motors, located directly upwind and upriver on the United States side of the border. These hyper-persistent chemicals bioaccumulated aggressively in the St. Lawrence River’s aquatic food web. Because traditional Native diets and cultural practices relied heavily on locally caught fish, the bioaccumulation of PCBs in aquatic life translated directly into hazardous human body burdens. Epidemiological studies, community health assessments, and blood tests conducted on tribal members have consistently shown elevated PCB levels. These specific toxicological burdens are negatively associated with proper thyroid hormone function, healthy neurological development in children, and an increased risk of severe chronic diseases. Notably, the IARC confirms that PCBs increase the risk of developing malignant melanoma, non-Hodgkin lymphoma, and breast cancer, directly linking the upstream pollution to the downstream oncological reality.
The resulting health advisories, which outright forbade the community from eating the fish they had relied upon for thousands of years, forced a rapid, unnatural dietary shift. Akwesasne residents were compelled to transition to a “Western” diet with a heavy reliance on processed fats and refined sugars to avoid PCB toxicity. This forced ecological severance generated secondary, devastating health crises within the community, including explosive rates of diabetes, obesity, and cardiovascular disease. This dynamic vividly illustrates the cascading, multi-generational impacts of environmental degradation, where the eradication of a traditional food source spawns an entirely new matrix of metabolic diseases.
Evaluating the Hydrological Hypothesis: Municipal Drinking Water
Given the expansive, undeniable contamination of the St. Lawrence River sediment and the local terrestrial brownfields, residents logically formulate the hypothesis that the municipal tap water must serve as a primary vector for carcinogens. However, to evaluate this scientifically, one must sharply and categorically differentiate between the raw environmental water flowing in the St. Lawrence River, the contaminated sediment residing in the riverbed, and the highly treated municipal drinking water supplied directly to Cornwall homes.
A thorough review of contemporary water quality data and regular statutory testing at the Cornwall municipal intake confirms that there are absolutely no current issues adversely impacting the source water used for the city’s drinking supply. The City of Cornwall’s Water Purification Plant utilizes a robust, multi-barrier approach to water treatment that is specifically engineered to eradicate both biological and chemical threats.
The initial phases of treatment include coagulation, settling, and intensive filtration, which effectively remove particulate matter and suspended solids from the raw river water. Following filtration, the water is subjected to primary disinfection using Ultraviolet (UV) light technology. UV disinfection is highly advanced; it penetrates the cellular walls of microorganisms, disrupting their DNA and ensuring the absolute destruction or inactivation of harmful pathogens (like Cryptosporidium and Giardia) which are often too small to be removed by standard mechanical filtration. Furthermore, the city utilizes sodium hypochlorite (a liquid form of chlorine) for primary chlorination and secondary disinfection. This ensures that a measurable residual concentration of free chlorine is maintained throughout the entire span of the city’s distribution system, effectively preventing any bacterial regrowth within the pipes and providing an immediate, measurable metric to detect any unexpected changes in water quality.
Regarding the specific concern of chemical carcinogens, municipal drinking water systems in Ontario are strictly regulated under rigorous provincial standards. The heavy metals (like mercury and zinc) and complex organic compounds (like PAHs and PCBs) that bind to the sediment in the riverbed are predominantly hydrophobic in nature; they cling tenaciously to soil particles and do not readily dissolve into the flowing water column unless physically disturbed. Because the Cornwall municipal intake draws from the flowing water column and the purification plant’s filtration and coagulation protocols are highly effective at screening out sediment-bound particulate matter, these specific legacy toxins do not enter the municipal supply.
Consequently, the hypothesis that current municipal tap water is the primary causative agent for the elevated incidence of early-onset and general cancers in Cornwall is completely unsupported by toxicological chemistry, municipal monitoring data, and hydrological science. However, a critical caveat remains: individuals who routinely consume sport fish caught directly from the Area of Concern, or individuals who frequently wade in and are exposed to untreated river water and sediment near historical discharge zones, face entirely different and potentially dangerous exposure pathways. Health advisories limiting the consumption of certain local fish remain a mandatory and critical public health defense mechanism in the region.
Air Quality, Respiratory Morbidity, and the Latency of Disease
If the municipal water supply is biochemically exonerated, the investigation must pivot to ambient air quality, evaluating both historical respiratory burdens and present atmospheric conditions.
Historically, Cornwall suffered from phenomenally severe air pollution, driven directly by the colossal emissions of the domestic pulp, paper, and chemical industries. In 1995, an investigation by Health Canada reported that the rate of hospitalization for severe asthma in Cornwall was approximately double that of other major, heavily industrialized Ontario cities such as Hamilton, Sudbury, and Windsor. Even more tragically, clinical research demonstrated that infants under two years of age residing in Cornwall experienced four times the expected hospital admission rate for acute asthma and respiratory distress. The ceaseless industrial emissions, characterized by the daily atmospheric release of acidic vapors, highly abrasive fine particulate matter, and sulfurous compounds, fueled widespread, justified public health terror regarding respiratory diseases and lung cancer.
However, the epidemiological landscape began to shift following deindustrialization. The permanent shutdown of the Courtaulds rayon operation in 1992, followed by the closure of the massive Domtar paper mill in 2006, catalyzed a drastic, measurable improvement in local air quality. Today, Cornwall consistently ranks in the top tier of monitored communities across Ontario for clean air, with recent studies ranking its air quality highly among comparable municipalities. Current levels of nitrogen dioxide (NO2), ozone, and fine particulate matter (PM2.5) across Ontario have seen substantial, permanent reductions over the past decade. These improvements are largely driven by aggressive provincial air quality initiatives, most notably the total phase-out and banning of coal-fired electricity generating stations in the province, as well as significantly stricter emission controls on vehicles and remaining industries. While southwestern Ontario still grapples with transboundary smog and ozone pollution drawn across the border from industrialized US cities during hot summer weather patterns, Cornwall’s localized industrial smog has largely dissipated.
This historical context is the skeleton key to understanding the current cancer data. Carcinogenesis, particularly for lung and rectal cancers, features an extensive latency period that can easily span 15 to 30 years from the point of initial chronic exposure to the manifestation of terminal disease. Therefore, the significantly elevated lung cancer incidence and mortality currently observed in the older demographics within Cornwall and the EOHU does not reflect the clean air of 2026. Rather, it represents the delayed, tragic epidemiological manifestation of the severe, highly toxic air pollution inhaled by residents during the 1970s, 1980s, and 1990s.
Lifestyle Covariates: Tobacco Consumption and Synergistic Risks
While legacy environmental pollution represents a significant, undeniable hazard, extensive public health analyses consistently and uniformly demonstrate that behavioral risk factors—primarily the consumption of combustible tobacco—are the absolute most dominant drivers of specific regional cancer spikes, routinely overwhelming ambient environmental exposures in predictive statistical models.
To quantify this, Public Health Ontario rigorously estimates the annual environmental burden of cancer for the province. Their models attribute roughly 2,090 to 2,990 new cancer cases provincially to UV radiation exposure, 1,080 to 1,550 cases to indoor radon gas, and a comparatively smaller 290 to 900 new cancer cases to fine particles in ambient air pollution (PM2.5). In stark, undeniable contrast, tobacco smoking is singularly responsible for tens of thousands of newly diagnosed malignancies and subsequent deaths annually.
When evaluating the Eastern Ontario Health Unit, the data regarding tobacco use is highly concerning. Smoking prevalence within the EOHU is profoundly elevated compared to the rest of the province. Extensive data derived from the Canadian Community Health Survey (CCHS) indicates that the prevalence of current smoking in the EOHU population stood at 23.5%, a figure significantly higher than the overall Ontario provincial average of 18.1%. Other historical iterations of the survey have captured EOHU smoking rates reaching as high as 27.2%, consistently and repeatedly flagging the eastern region as harboring higher-than-average, entrenched tobacco consumption.
The epidemiological correlation here is impossible to ignore. The significantly elevated rates of lung cancer incidence (99.6 per 100,000 for EOHU males versus 82.2 provincially) and lung cancer mortality (79.9 per 100,000 for EOHU males versus 60.2 provincially) map flawlessly onto these elevated regional smoking rates. Combustible tobacco is not only the primary, overwhelming cause of lung cancer, but it is also recognized as a major independent risk factor for the development of colorectal cancer, explaining the dual spike of these specific malignancies in both male and female populations in the EOHU.
Furthermore, the interplay between environmental contaminants and lifestyle factors produces deadly synergistic effects. For example, exposure to indoor radon gas—a naturally occurring radioactive gas that seeps into residential basements from the underlying bedrock—is recognized by Health Canada as the second leading cause of lung cancer. However, the risk of developing lung cancer from residential radon exposure is magnified exponentially if the exposed individual is also a smoker. While comprehensive geographical studies investigating radon in areas like Devon and Cornwall in the UK have shown varying, sometimes inconclusive impacts on baseline lung cancer mortality , the core toxicological principle remains absolute: underlying environmental risks in Cornwall, Ontario, whether stemming from legacy industrial dust, historical air quality, or highly localized indoor radon, are catalyzed into fatal malignant outcomes at vastly higher rates in populations that feature heavily elevated smoking prevalence. Similarly, the sharply rising colorectal cancer rates observed in young people under forty are tightly intertwined with the measured 1.9% annual increase in youth obesity and the widespread adoption of sedentary lifestyles , representing critical covariates that must be considered alongside any environmental hypothesis.
Remedial Interventions and Ecosystem Surveillance
Recognizing both the elevated cancer burden and the permanent legacy of industrial ecotoxicity, healthcare and environmental institutions in the Cornwall region are proactively executing highly targeted countermeasures.
To directly combat the disproportionate, preventable lung cancer mortality rates, specialized lung cancer screening pilot programs have been actively deployed. Cancer Care Ontario has initiated a high-risk lung cancer screening program utilizing a strategic “hub-and-spoke” model. Within this framework, major facilities like The Ottawa Hospital serve as the central hub, while the Cornwall Community Hospital operates as an integrated spoke site. This infrastructure enables highly vulnerable individuals—such as long-term heavy smokers—to access advanced low-dose CT scans much closer to home. By utilizing sophisticated imaging to identify asymptomatic lung tumors at earlier, highly treatable stages, these specific clinical initiatives aim to drastically reduce the potentially avoidable mortality rate that currently plagues the region.
Simultaneously, environmental vigilance in Cornwall is spearheaded by the St. Lawrence River Institute of Environmental Sciences. Established in 1994 and located directly on the local college campus, this independent, not-for-profit research facility conducts highly advanced ecotoxicological research on large freshwater river ecosystems. Their mandate ensures that legacy contaminants, specifically the mercury and PCBs buried in the riverbed, are continuously monitored to prevent their lethal re-entry into the local food web.
In a powerful demonstration of ecological collaboration, the River Institute, partnering closely with the Mohawk Council of Akwesasne, currently leads the “Great River Rapport”. This initiative is an exhaustive, community-based ecosystem health report that systematically assesses 35 distinct indicators of ecological health for the Upper St. Lawrence River. By synthesizing rigorous, science-based empirical data with Indigenous knowledge and perspectives, this project accurately tracks fish contamination levels and ambient water quality, providing the crucial, real-time data required to inform local public health advisories and dictate long-term environmental remediation strategies. Their ongoing, relentless surveillance provides a vital scientific safeguard, ensuring that the mandates of the Cornwall Sediment Strategy operate exactly as intended, and that legacy contaminants remain permanently buried and biochemically inert.
Conclusions
An exhaustive, rigorous review of the epidemiological, environmental, and public health data concerning the municipality of Cornwall and the encompassing Eastern Ontario Health Unit yields several definitive, scientifically substantiated insights regarding the community’s cancer burden.
First, the EOHU, which includes Cornwall, definitively exhibits statistically significant elevations in both the incidence and mortality of lung and colorectal cancers when compared directly to the Ontario provincial averages. Consequently, Cornwall’s Potentially Avoidable Mortality (PAM) rate is nearly double the provincial benchmark for both men and women, signifying severe, deeply entrenched systemic health vulnerabilities within the local population.
Second, the deeply tragic deaths of young individuals under the age of forty from cancer reflect a much broader, continent-wide epidemiological shift rather than a highly localized toxic event. Early-onset breast cancer and early-onset colorectal cancer are rising sharply across all of Canada. This rise is driven heavily by systemic lifestyle shifts, steadily rising obesity rates, and evolving biological factors that are currently prompting provincial health authorities to rapidly lower the ages of eligibility for life-saving screening programs. While deeply felt and mourned at the local level, this specific phenomenon is not a statistical anomaly isolated to the geography of Cornwall.
Third, while Cornwall undeniably possesses a heavy, highly toxic industrial legacy—evidenced by the PAHs, PHCs, and heavy metals saturating sites like the former Domtar mill, and the legacy mercury and PCBs embedded in the St. Lawrence River bed —the municipal drinking water is biochemically safe. The Cornwall Water Purification Plant utilizes highly advanced UV disinfection and chemical chlorination protocols, and routinely tests negative for raw water pathogen or chemical issues. Because the legacy toxins are predominantly bound to the river’s benthic sediment and do not suspend readily into the municipal intakes, the hypothesis that current tap water is driving the regional cancer rates is scientifically unsupported.
Ultimately, the true, data-driven drivers of Cornwall’s elevated cancer rates are a deadly combination of extremely high regional smoking prevalence—which sits far above the provincial average—and the delayed, tragic manifestation of diseases caused by historical air and occupational pollution inhaled during the 1970s through the early 2000s, prior to the total closure of the city’s major industrial polluters. The path forward for the community relies inherently on maximizing participation in early-detection screening programs (such as the newly expanded colorectal guidelines and targeted low-dose lung scans) and maintaining the aggressive, ongoing environmental surveillance pioneered by entities like the River Institute. Through dedicated behavioral public health interventions and strict, unforgiving environmental stewardship of terrestrial brownfields, the region can actively mitigate its heavy historical burdens and safely reshape its future epidemiological profile.
Sources
Exhaustive Investigatory Bibliography
A complete compilation of all cited data registries, scientific journals, news reports, and environmental assessments relating to cancer incidence and environmental factors in and around Cornwall, Ontario.
Sources are categorized by thematic relevance to assist in cross-referencing public health outcomes with legacy industrial and environmental data.
1. National & Provincial Cancer Statistics
| Domain / Provider | Report / Title |
|---|---|
| cancercareontario.ca | Ontario Cancer Statistics 2024 |
| cancercareontario.ca | Ontario Cancer Statistics 2022, Key Findings |
| cancercareontario.ca | Ch 1: Estimated Current Cancer Incidence [2022] – Cancer Care Ontario |
| cancercareontario.ca | Ch 4: Cancer Incidence [2022] – Cancer Care Ontario |
| cancercareontario.ca | Ontario Cancer Statistics 2022 Data Sources |
| cancercareontario.ca | Ontario Cancer Statistics 2018 |
| cancercareontario.ca | Cancer statistics by public health unit – Cancer Care Ontario |
| cancercareontario.ca | ONTARIO CANCER STATISTICS |
| www150.statcan.gc.ca | The Daily — Cancer incidence in Canada, 2022 |
| cancer.ca | Cancer statistics at a glance | Canadian Cancer Society |
| canada.ca | ARCHIVED – Chronic Diseases in Canada |
| eohu.ca | Health Indicators (Eastern Ontario Health Unit) |
2. Emerging Trends: Youth Cancer Demographics
| Domain / Provider | Report / Title |
|---|---|
| uottawa.ca | Breast cancer rates rising among Canadian women in their 20s, 30s and 40s |
| canadianaffairs.news | New data show where breast cancer rates are highest |
| badgut.org | Colorectal Cancer on the Rise in Young Adults |
| news.ontario.ca | Ontario Lowering Eligibility Age for Life-Saving Colon Cancer Screening |
3. Environmental Legacy & The St. Lawrence River
| Domain / Provider | Report / Title |
|---|---|
| canada.ca | St. Lawrence River at Cornwall/Akwesasne: Area of Concern – Canada.ca |
| ijc.org | St. Lawrence River – Area of Concern Status Assessment – International Joint Commission |
| extapps.dec.ny.gov | St. Lawrence River Area of Concern Status Assessment |
| riverrapport.ca | Region – The Great River Rapport |
| rrca.on.ca | Sediment Strategy – Raisin Region Conservation Authority |
| standard-freeholder.com | Contaminants of concern identified at Lock 18, former Domtar site… |
| standard-freeholder.com | Cornwall councillors query River Institute staff on legacy contaminants, microfibres |
| watertoday.ca | cornwall triathlon: is it time to pull our heads out of the sediment? |
| pubs.acs.org | Downwind Distribution of All-Cancer Relative Risk about a Point Source: Single Source with Reactive and Unreactive Plumes |
| en.wikipedia.org | Courtaulds – Wikipedia |
| en.wikipedia.org | Cornwall, Ontario – Wikipedia |
4. Akwesasne Mohawk Studies & Local Research Institutes
| Domain / Provider | Report / Title |
|---|---|
| pmc.ncbi.nlm.nih.gov | Health Disparities and Toxicant Exposure of Akwesasne Mohawk Young Adults: A Partnership Approach |
| digitalcommons.usu.edu | “Environmental Contamination at Akwesasne” by Thoin F. Begum, David O. Carpenter et al. |
| srmt-nsn.gov | Saint Regis Mohawk Tribe Joins Lawsuit Against Monsanto Corporation |
| extapps.dec.ny.gov | Xenobiotics in Fish from the St. Lawrence River and Connecting Tributaries |
| facetsjournal.com | Governing for transboundary environmental justice: a scientific and policy analysis of fish consumption advisory programs |
| perchmagazine.com | The Bridge: Abraham Francis – Perch magazine |
| riverinstitute.ca | The River Institute |
| riverinstitute.ca | Ecosystem Health Report – The River Institute |
| b2match.com | ST LAWRENCE RIVER INSTITUTE OF ENVIRONMENTAL SCIENCES |
5. Air Quality, Drinking Water, Radon & Lifestyle Risk Factors
| Domain / Provider | Report / Title |
|---|---|
| cornwall.ca | 2024 Drinking Water Quality Report |
| yourdrinkingwater.ca | CORNWALL – Protect Your Drinking Water |
| ontario.ca | 10-year trends and annual results | Air Quality in Ontario 2023 Report |
| airqualityontario.com | Air Quality in Ontario Report 2016 |
| iqair.com | Ontario Air Quality Index (AQI) and Canada Air Pollution |
| publichealthontario.ca | Environmental Burden of Cancer | Public Health Ontario |
| pmc.ncbi.nlm.nih.gov | Utility gains from reductions in the modifiable burden of lung cancer attributable to residential radon in Canada |
| cbc.ca | Radon gas levels in homes need to be checked, lung cancer experts say |
| stacks.cdc.gov | Radon and Cancers Other Than Lung Cancer in Underground Miners |
| www150.statcan.gc.ca | Bronchus and lung cancer incidence… age-standardized rate per 100,000 population, 2000 |
| otru.org | CCHS Data on Smoking Prevalence and Secondhand Smoke Exposure in Ontario |
| www150.statcan.gc.ca | Table 2. Percentage of current smokers, by province/territory and health region, 2005 |
| www150.statcan.gc.ca | Findings from the Canadian Community Health Survey (CCHS) – Smoking and Diabetes Care |
| s22457.pcdn.co | Lung Cancer Screening in Canada |
Note on Cross-Jurisdictional Search Results
The initial data gathering also surfaced studies and programs related to Cornwall, United Kingdom, largely due to shared nomenclature and shared variables (like Radon tracking). These have been isolated below for transparency.
| Domain / Provider | Report / Title |
|---|---|
| ideas.repec.org | Radon and Lung Cancer in Cornwall and Devon – IDEAS/RePEc |
| pubmed.ncbi.nlm.nih.gov | An ecological study of cancer incidence and radon levels in South West England |
| peninsulacanceralliance.nhs.uk | More than 50,000 in Cornwall, Isles of Scilly to be invited for NHS lung health checks |
| england.nhs.uk | Life-saving lung checks reach milestone in Cornwall with 6000th person scanned |